
Final Answers vs. First Principles: What JAMA’s Benchmark Reveals
Recent work in JAMA Network Open introduced the PrIME-LLM benchmark to test how large language models handle real clinical reasoning, not just exam-style questions. Researchers evaluated 21 off-the-shelf systems on 29 vignettes, scoring them across differential diagnosis, diagnostic testing, final diagnosis, management, and miscellaneous reasoning. The headline result: models were far better at naming a final diagnosis than at generating broad, safe differential lists. Failure rates for differential diagnosis exceeded 0.80 across all models, while they dropped below 0.40 for final diagnosis. In other words, once the case was almost solved, models looked impressive; at the messy, ambiguous beginning, they struggled. Reasoning-optimized models and GPT variants performed best overall, and most systems improved when given images as well as text, underscoring the promise of multimodal AI healthcare tools—but also their current limitations in early, hypothesis-driven thinking.

Where Multimodal AI Healthcare Is Already Delivering Value
Healthcare software developers are betting heavily on multimodal AI healthcare platforms that fuse imaging, clinical notes, lab results, genomics, and wearable streams. Unlike earlier systems that focused on a single data type, these models integrate diverse inputs to create a more holistic picture of patient health. This is particularly attractive for precision medicine, where tailoring therapy to genetics, lifestyle, and longitudinal clinical history demands cross-modal insight. Hospitals and clinics are shifting from pilots to production-grade clinical decision support AI, using multimodal systems to prioritize scans, flag subtle patterns in imaging, and surface at-risk patients based on combined sensor and record data. These applications play to AI’s strengths: high-volume pattern recognition and consistent application of guidelines. Yet they mostly sit downstream in the workflow—augmenting specialist review and triage—rather than replacing clinicians’ early-stage reasoning or nuanced differential diagnosis.
Overconfidence and the Limits of AI Differential Diagnosis
The PrIME-LLM results highlight a structural problem: current models excel when the answer space is narrow but falter when uncertainty is high. In differential diagnosis, safe practice demands broad, prioritized lists that keep rare but dangerous conditions in play. LLMs, however, often collapse too quickly onto a single plausible label, especially when prompted to behave like confident experts. This overconfidence is risky in real-world medicine, where incomplete histories, atypical presentations, and conflicting data are the norm. Even when multimodal inputs such as images boost accuracy, the underlying reasoning can remain brittle. Models may appear rigorous by echoing clinical language while simply matching patterns in training data. Asking them to "think like doctors" exposes gaps in causal reasoning, test selection, and management planning—areas where human clinicians balance probabilities, costs, patient values, and safety margins in ways today’s systems cannot reliably emulate.
Youth Mental Health: Powerful Signals, High Stakes
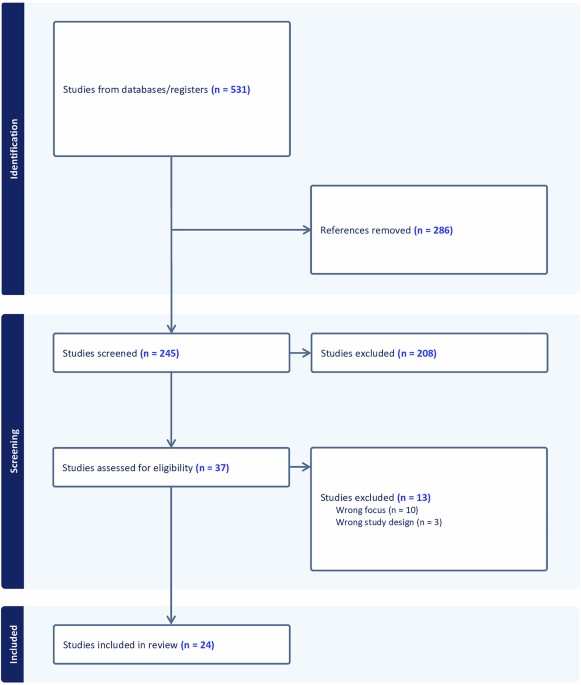
Youth mental health AI tools illustrate both the promise and peril of multimodal approaches. A recent scoping review identified only 19 studies directly addressing youth mental health with AI, yet many already combine physiological signals, smartphone and wearable data, self-reports, and social media or app-derived features. Online learning methods allow models to adapt over time, track stress trajectories, and cope with concept drift as students’ routines and environments change. Systems such as branched deep learning architectures on datasets like StudentLife and WESAD show strong stress classification performance using continuous multimodal streams. However, this domain is highly sensitive: misclassification can trivialize serious distress or over-pathologize normal fluctuations. The heterogeneity of data, the need to handle cold start users, and the ethical weight of monitoring minors underscore why mental health AI tools must be framed as supportive monitoring and triage aids, not autonomous diagnosticians or therapists.
From Second Opinions to Safer Systems: Guardrails and Next Steps
For now, multimodal clinical decision support AI should be treated as a second opinion and triage partner, not a primary decision-maker. Hospitals can embed these systems to pre-screen imaging, flag concerning combinations of labs and vital signs, or suggest possible diagnoses that clinicians can confirm or discard. Clear policies should forbid unsupervised use in complex, ambiguous presentations, particularly in youth mental health and other sensitive areas. Vendors and health systems need robust evaluation frameworks like PrIME-LLM that test longitudinal reasoning, not just final-answer accuracy, and they must calibrate models so confidence scores better reflect true uncertainty. Future progress will depend on richer, more representative training data, stronger multimodal integration, and online learning methods that safely handle concept drift without compromising reliability. Until those pieces are in place, the safest path is to let multimodal AI extend clinicians’ reach while keeping humans firmly in charge of the diagnostic journey.